
Abstract
Growing evidence suggests that images in medical teaching materials could potentially be providing a
representation of illness that is narrow and incomplete. Accordingly, this opinion piece will explore
implications for under-represented demographic groups. The resulting gulf in health care outcomes, delayed diagnosis, and missed diagnosis are likely to have multiple contributing factors, including poorer access to medical intervention and ‘multiple disadvantage’. The lack of diversity depicted in medical textbooks is also a possible contributing factor that could shape the expectation of physicians. As such, this article explores the range of medical illustrations used in popular medical textbooks. The topic of medical illustration and under representation is of specific relevance to the JBIMA readership. Both cultural and religious reasons are probable for the hesitancy in consenting to photography for educational purposes – due to the concept of awra in Islamic tradition. Furthermore, we explore if the lack of volunteers from ethnic groups to be the subject of medical photographs in textbooks could also play a role. Finally, to encourage participation, ethical concerns related to clinical photography are discussed from an Islamic viewpoint.
Background
Unconscious assumptions can play an important role in many aspects of medicine, including the recruitment of future physicians and their journey to qualified status. Accumulating evidence shows that the stereotype of medical doctors is predominantly one of white-males For example, Freedom of Information requests gathered by the British Medical Journal revealed that white candidates working in London were six times more likely to be offered a job in medicine than black applicants[1] Such representations are not only unjust, but appear to make medicine less accessible not only for patients of diverse backgrounds but even for students interested in pursuing a career in medicine. Moreover, authors of medical textbooks are becoming increasingly aware that different skin tones are poorly represented leading to inaccurate, in addition to, delayed diagnoses. The editor of the Journal of Visual Communication in Medicine, Erolin, noted that ‘… an area of growing concern for many students is the apparent gender and race bias still visible in many contemporary anatomical textbooks’ [2].
Furthermore, in the 2021 edition of the popular textbook, First Aid, the editors reported an internal audit of previous editions. They noted that the illustrations had scarce representation of females, as well as a limited range of skin tones [3]. Additionally, in the 2021 foreword, the authors concluded that the 2020 edition contained 70 illustrations in total – all described as ‘male appearing’ and depicting skin tones that were ‘pink’ or ‘light beige’ [3]. First Aid has consequently committed to including medical illustrators that would show greater gender representation and a wider range of the Fitzpatrick skin typesI-VI [3].
Despite many clinicians and academics being determined to implement significant change, the current lack of diversity is problematic for multiple reasons. First, let us consider the way change is actively hindered. Many industries appear to portray a certain perception about who leads the profession and shapes the future; such leaders are given an image, a so-called face – creating a stereotype. Despite demographic facts contradicting expectations, challenging such stereotypes and the existing hegemony can be a slow and difficult process [4]
In the 2008 text The Changing Face of Medicine, boulis and Jacobs observed that since the 1960s the medical profession in the US has attracted significantly more women. The authors argue that this evolution reflects social changes in everyday American society and is multi-directional, in that increased participation changed the industry and adjusted the status and roles of women beyond medicine [5]. The Association of American Medical Colleges (AAMC) revealed that there are now more female medical school applicants than males. However, Michael Dill, AAMC’s director of workforce studies, comments: ‘If the majority of female physicians are still concentrated in a handful of specialities, then we haven’t gotten where we need to be’ [6]. Despite these demographic shifts within the medical profession, the so called face is still male and still white.
In the UK, application data compared over the last 50 years has revealed a trend towards increasing diversity [7]. Moreover, researchers observe that in comparison to other undergraduate disciplines, medicine has greater diversity [8]. However, rising numbers of non-white graduates alone will not lead to meaningful change. A greater problem appears to be the organisational culture, which is fraught with hidden obstacles that hinder progression for non-white clinicians and lead to disciplinary hearings that are disproportionate. In the UK, the General Medical Council has been recently criticised by the British Medical Association for their inadequate support of non-white doctors [9]. Accordingly, to achieve the aim of a medical workforce that represents the population it treats, the NHS has yet to make sufficient progress.
Furthermore, the lack of representation has clinical implications. Within medicine, a lack of visible diversity in healthcare providers has serious and significant consequences for patient outcomes and staff welfare [10][11][12]. Accurately diagnosing diseases for patients of certain ethnic groups, for instance, remains a known problem. This concerning phenomenon is apparent in many disciplines, including psychiatry. In the interpretation of affective disorder symptoms, researchers have observed that in relation to schizophrenia, the diagnosis was applied significantly more frequently to African American men [13][14].
In recent years, academic journals have been examined to reveal the degree of inclusion therein of patients from a more ethnically diverse sample. For example, over 25,000 colour photographs and colour illustrations in leading plastic surgery journals were categorised according to the Fitzpatrick scale and then entered into regression analysis [15]. The analysts reported that only 22% of all images sampled between 1992 and 2017 were from Fitzpatrick skin types IV=VI as opposed to I-III i.e., the vast majority of images depicted white skin tones. Moreover, when the proportion of images used in each academic article was considered, the categories were disproportionate, with non-white skin featuring a mean of 1.6 times per article and white skin 5.4 times [15].
Other areas of medicine in which researchers have established a pattern of increased risk and delayed diagnosis along ethnic lines include dermatology [16], oncology [17], and obstetrics and gynaecology [18]. For example, the occurrence of cancer is generally lower in the UK for non-white individuals [19]. However, outcomes are disproportionally poorer. In the UK, diagnoses for breast cancer appear to be made in later stages for women from ethnic minorities[17]. Moreover there is evidence that symptoms can be misinterpreted, underplayed, or even ignored leading to deadly consequences. Similarly, the high rates of maternal mortality in women of colour in the UK and USA have been the focus of books, documentaries, and extensive articles and have been termed national scandals [20] [21] [22] .
On the note of significant underrepresentation, scrutiny of medical journals related to breast surgery revealed a paucity of non-white patient images [23]. Likewise, The Lancet published a systematic review of publicly available skin cancer images revealing that fewer skin samples were taken from Fitzpatrick skin types IV-VI [24]. This pattern has also been observed in dermatology journals [25]. However, within academia and wider society, there has been increasing focus on health inequalities and the poor representation of non-white patients has gained attention. Policies have been implemented to improve representation.
Changing the stereotype of a medical doctor from that of someone white and male and representing doctors from a range of diverse backgrounds could make medicine more inviting; especially to other races. The set of assumptions about the race of doctors and patients is pervasive and problematic on multiple levels. Researchers have also observed a recruitment ‘snowball effect’ in which greater representation leads to increased diversity in the pool of applicants [26]. Consequently, a diverse representation of medical doctors would also increase trust in patients of diverse backgrounds. An increase in patient trust could cultivate greater trust in clinical photography and the use of photographs for medical research and medical textbooks.
Applications of medical illustration and clinical photography
On both sides of the Atlantic, creating medical artwork requires significant training and the professional practice is regulated. In the USA, for instance, the Association of Medical Illustrators (AMI) oversees the accreditation of individual professionals. Training courses in medical illustration, on the other hand, are accredited by the Commission on Accreditation of Allied Health Education Programs (CAAHEP). Similarly, in the UK, medical illustration (drawings and photography) is regulated and professional clinical photographers are provided with extensive guidance. Guidance on inclusion, accessibility, and sensitive working practices, for instance, is provided by IMI, the Institute of Medical Illustration.
The journey towards full inclusivity is acknowledged as an ongoing endeavour and the IMI is open to recommendations from both clinicians and patients. The IMI website states: We welcome your comments or suggestions for improvements to these guidelines. If you have any suggestions for existing guidelines, or wish to be involved in a working group for any new guidelines, please contact the National Guideline Coordinator,Larissa Lee [27].
Before we move on to solutions, let’s take a brief look at the history of medical images. Before the invention of the camera obscura, the main tool available to teachers and trainee physicians was anatomical sketches. Notably, the Association of Medical Illustrators [28] observed that medical illustrations have existed for over 2000 years. In Hellenic Alexandria, Egypt between the 3rd and 4th Century BC, evidence from sheets of papyrus suggests that medical illustrations for teaching purposes were sketched [28].
From the 20th Century onwards medical images took the form of either photographs or drawings. The uses of these images range across various purposes including patient information, medical and anatomical education, scientific communication, professional exhibits, and even for advertising pharmaceutical and medical equipment. Consequently, a vital medium for doctor-patient communication, scientific innovation and disease management has been medical images. Table 1 below summarises some of the purposes for illustrating various anatomical regions in medical teaching materials.
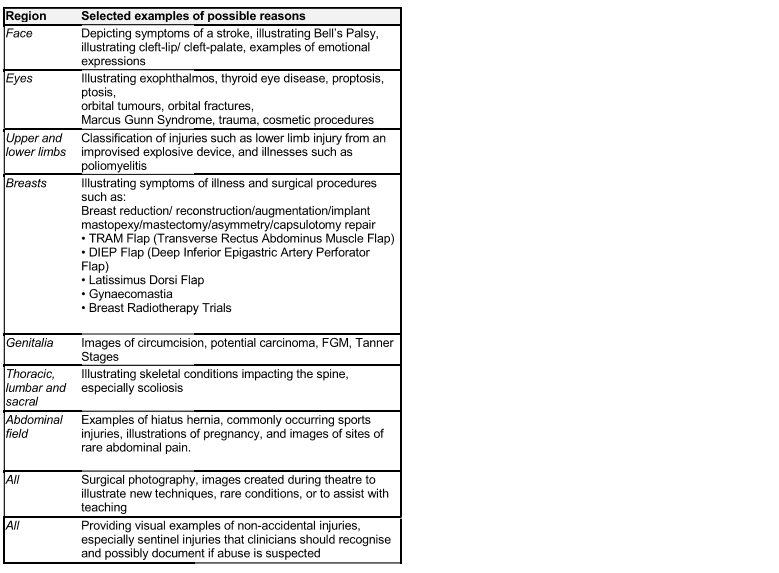
A cursory glance at the content that is illustrated in medical textbooks raises ethical questions about the sensitive nature of the images. Although the table is not intended to be exhaustive, it does convey the wide range of medical illustrations students would be expected to encounter during their medical education. From an Islamic medical viewpoint, the use of such images requires addressing some ethical concerns.
Medical Textbooks
A brief review of the literature revealed that general medical textbooks are also experiencing a lack of non- white illustrations. Academic journals are typically published more frequently than textbooks and we would assume that they would be quicker to implement new policies on inclusion. Louie and Wilks [29] appraised images from four popular medical textbooks for students:
1) Atlas of Human Anatomy, 2) Bates’ Guide to Physical Examination & History Taking, 3) Clinically Oriented Anatomy, and 4) Gray’s Anatomy for Students. In total 4146 images were classified according to race and skin tone. The study concluded that images in these textbooks followed the approximate racial distribution of the USA: 62.5% White, 20.4% Black, and 17.0% person of colour. Nevertheless, with regard representation of skin tone, these influential medical textbooks showed an overrepresentation of lighter skin tone. The data showed that lighter skin tones were featured in 74.5% of the images, with 21% featuring medium tones and only 4.5% of the medical images featuring skin categorised as dark. Alarmingly, of the six types of cancers commonly occurring in people of colour, the textbooks provided no related images [29].
Moreover, despite observations that many regions around the world are becoming more ethnically diverse, dermatology textbooks rarely feature non-white skin[0] Such lack of inclusion is deeply concerning because popular medical textbooks are not illustrating the way common skin conditions could present in darker skin. Consequently, in relation to their non-white patients students may fail to identify acne vulgaris and pityriasis rosea. Furthermore, images of conditions such as erythema dyschromicum perstans which has a disposition associated with race were also rarely featured within the four sampled textbooks. Perhaps more concerningly, another observation found that certain infectious diseases were not represented in all skin tones. Such depiction could potentially create bias in future physicians to associate illnesses, such as syphilis, with patients with darker skin types [30].
Similarly, gynaecology textbooks are more likely to include images of Fitzpatrick skin types I-III or skin classified as light [31]. An analysis of vulvar conditions (VCs) depicted in major gynaecology textbooks aimed at the medical student market revealed that the images were significantly less likely to include darker skin tones [31]. The alarming trend of bias was apparent yet again with fewer images of VCs but a significantly higher number of images showing infectious conditions in darker skin tones [31].
In summary, there is growing awareness and intention to address the poor representation of clinical images in textbooks and journals. However, the current picture does not represent our UK patients. Such trends are concerning because the images to which medical students are exposed could unknowingly shape their expectations. As a result, later on in their careers, physicians might misdiagnose patients of colour or unconsciously associate them with stigmatising conditions.
Shariah-compliant clinical photography
We now move on to summarise the main ethico-medical issues when it comes to satr al-awra. As JBIMA largely serves a UK readership, we will provide principals according to the Sunni Hanafi school of thought, as this philosophy has the largest following in the UK. Understanding the Islamic viewpoint on photography is important for HCPs if health care is to improve. Cho et al. [23] highlight the importance of cultural competence for HCPs, ‘As surgeons, we have a responsibility to ensure that our trainees are not only technically but also culturally competent and that all our patients feel welcome and well represented by our specialities’ [23]. In this section, we will briefly recap and explore the implications of Shariah law regarding medical images. In a nutshell, Muslims who choose to adhere to rules of modesty and rules pertaining to mixed-gender interactions, commonly observe the practice of ‘satr al awra’. Linguistically, satr means to cover and awra means a secret or a hidden place, in this context meaning parts of the body that require to be concealed.
The main reason for Muslims to observe satr al awra is to have the right to cover areas of the body to maintain dignity. Other reasons could include preventing potential embarrassment or preventing covetousness as a result of exposure; which according to Shariah law, are considered to be harmful to a person’s spiritual health [32]. The aim of satr al-awra is also to minimise vanity, and rather than emphasise appearances, the emphasis is placed on people’s actions. For simplicity, Shariah law permits exposing parts of the body for convenience, especially where no harm is expected. Adult Muslim males consider the area of their bodies from the navel to the knees to be the awra. By contrast, bearing in mind the difference of opinions, adult Muslim females may consider their entire bodies as awra except for the face, hands, and feet. This understanding of the awra is a simplification for practical purposes of which clinical photographers need to be aware. The details of the topic of the awra can be found in manuals of Islamic Jurisprudence; also refer to Ibn Adam [33].
For clinical photography to be permitted in Shariah law, several factors need to be considered during the decision making process [34]. Intriguingly, the same concerns are considered during NHS guidance and ethical rules for clinical photography [27]. The key questions related to medical photography from an Islamic viewpoint are:
Is photography the only effective option?
What areas of the body are being photographed
Will the patient be identifiable?
Is the photography session, the manner of obtaining consent, storage, and the use of the photographs all Shariah-compliant?
Moreover, the doctor-patient relationship is generally that of a non-mahram nature, meaning that the patient and doctor are not blood relatives, nor are they immediate family. The question that arises from such a scenario, therefore, is how much of the body can a Muslim patient expose to non-family members? In this case, to the clinical photographer and to the HCPs who will have access to the photographs. The answer depends on the degree of need to expose particular areas of the body as well as the gender and sexual orientation of anyone looking at the patient. However, the anonymous nature of who will have access to the photographs makes the ethical status somewhat blurred.
Firstly, participating in photographs for a clinical need is acceptable when that is the only option for effective treatment. The permissibility is based on the idea that Shariah law encourages monitoring and maintaining health [35]. Likewise, photography for necessary matters such as passports and other forms of identification is also permitted for the sake of public safety, as well as for forensics to tackle crime [36].
The permissibility of digital photography was questioned by Muslim jurists only in the 19th century after advancements in camera technology [37]. Before that time, since the 7th century, concerns were raised mostly with regard to the permissibility of making sculptures and paintings of humans.
In any case, pornographic art in any shape or form has always been prohibited in Shariah law. Furthermore, describing a person’s body to a third party in a manner that sexually objectifies the subject or creates embarrassment for them is also prohibited. Such behaviour includes body shaming, which comes under the general prohibition of mockery and shaming (Qur’an, 49:11). For Muslim patients, therefore, clinical photography needs to follow particular rules and regulations for the patients to be assured that the process is Shariah-compliant
The ethical rules provided by the NHS and the IMI [27] are strikingly similar to the rules mandated by Sharia law. Accordingly, clinicians can help to ensure that certain measures are in place to minimise the misuse of images as well as minimise any risk or harm to patients. Bearing safeguarding measures in mind, the photographer needs to be reputable and preferably one that meets the requirements of the patient. Moreover, patients are likely to prioritise their dignity, safety, and well-being. As such, Muslim patients may wish to be accompanied by a trusted chaperone. Such measures could also prevent allegations of any inappropriate conduct.
Furthermore, photos should be used for purposes only to which the patient or their legal representatives consented in writing. If a photo contains the awra, then the patient should not be identifiable, i.e. the face should not be included in the photo, nor should any other identifiable features. If on the hand, a photo is taken of the an unidentifiable patient, then Hanafi jurists have excluded such images from prohibited art [38].
The precedent for such a ruling exists, for instance in the case of an amputated limb of an unidentifiable person. Likewise, Muslim jurists do not consider the reflection of an image to bear the same sanctity as the actual object it represents. Bearing these principles in mind, a clinical photograph is a) not the same as the patient themselves and b) the patient is to remain unidentifiable. The patient must be informed of the purpose of having their photos taken as well as the way their photos and their identity will be protected against any breach of confidentiality. The patient must also have the right to withdraw consent at any time.
Conclusion
The stereotype of medical doctors appears to be of white males. Such excluding representations are likely to impact different group members from diverse backgrounds; students seeking a career in medicine may feel less welcome whereas patients may be affected by an inaccurate or delayed diagnosis. Moreover, medical textbooks are currently not representative of darker skin tones leading to poor diagnoses of patients. Although this article is not a meta-analysis nor an exhaustive appraisal, we have used a hypothetical link to help understand a real social problem. Moreover, to improve representation, we encourage more patients to participate in clinical photography. As such, medical textbooks require improvement. Medical illustrations need to be more representative to make medical imaging more accessible for previously and currently less represented demographic groups. New more inclusive and encouraging policies associated with long-term and sustainable improvements could also be considered to allow a representation of a wider range of ethnicities in medical teaching materials.
Underrepresentation of skin tones as well as the misrepresentation of conditions found in darker skin tones affect not only ethnic minorities but clinicians in their practice. Improvements in representation in medical images could begin with doctors making patients aware of ways to participate in and contribute to clinical photography. A key message for the Muslim population needs to be that Shariah law provides scope to have clinical images taken especially when the strictest of ethical protections are applied. Current clinical photography practice appears to be Shariah-compliant Should more ethnicities consent for their images to be included in education materials, greater representation of ethnicities would be possible, which in turn makes medicine more inviting to all ethnicities as well as allow better opportunities for trainees to treat a diverse range of patients.
Moreover, interviews could also be conducted with Muslim patients to understand their views on allowing photography for medical research and textbooks. Female Muslim HCPs/patients, as well as those from different ethnicities, can make an informed decision about having their photos taken for clinical purposes whilst taking into account Shariah guidelines.
References
- Cunliffe, S. Race, Recruitment and Denial in the
NHS: An independent study of the likelihood of job-offer
from application by ethnicity, across the 18 NHS Acute
Trusts in London [pdf]; 2021, Oct [cited 2022, Nov 28].
Available from: https://citou. com/wp-content/uploads/2021/10/Race-and-Recruitment-Report-FINAL-2-10-21. pdf - Erolin, C. Medical Illustration in the 21st century and
beyond, Medical Writing. 2020, 29(1), 1-10 - Le, T., Bhusan, V., Sochat, M. First Aid for the
USMLE Step 1 2021: A student-to-student guide. New York: McGraw Hill; 2021. - Mills, A. J. Man/Aging Subjectivity, Silencing
Diversity: Organizational Imagery in the Airline
Industry. The Case of British Airways. In Albert M
(ed.). Insights and Research on the Study of Gender and
Intersectionality in International Airline Cultures.
Bingley: Emerald Publishing Limited; 2017. pp. 367-392 - Boulis, A. K. and Jacobs, J. A. The Changing Face of
Medicine: Women Doctors and the Evolution of Health
Care in America. The Culture and Politics of Health Care
Work. Ithaca, N. Y.: Cornell University Press; 2008. - Boyle, P. Nation’s physician workforce evolves:
More women, a bit older, and toward different specialties
[Internet]; 2021, Feb 2 [cited 2022, Nov 23]. Available
from:https://www. aamc. org/news-insights/nation-s-
physician-workforce-evolves-more-women-bit-older-
and-toward-different-specialties - Independent Reviewer on Social Mobility and Child
Poverty. Fair Access to Professional Careers: A progress
report by the Independent Reviewer on Social Mobility
and Child Poverty[pdf]; 2012, May [cited 2022, Nov 23].
Available from:https://assets. publishing. service. gov.
uk/government/uploads/system/uploads/attachment_data/
file/61090/IR_FairAccess_acc2. pdf - Universities UK. Patterns and trends in UK higher
education 2018 [pdf]; 2018 [cited 2022, Nov 23].
Available from: - https://www. universitiesuk. ac. uk/facts-and-stats/data-and-analysis/Documents/patterns-and-trends-in-uk-higher-education-2018. pdf
- Nagpaul, C. A landmark ruling, and why the GMC
must now ensure fairness for all [Internet]; 2021, June 25
(cited 2022, Dec 1). Available from: https://www. bma.
org. uk/news-and-opinion/a-landmark-ruling-and-why-
the-gmc-must-now-ensure-fairness-for-all - Moreno, N. A. Of Capes and White Coats:
Championing Diversity and Inclusion in Medicine.
Annals of surgery. 2021, 273(2), e32–e33 - Swartz, T. H., Palermo, A. S., Masur, S. K. and
Aberg, J. A. The Science and Value of Diversity:Closing
the Gaps in Our Understanding of Inclusion and
Diversity. The Journal of infectious diseases, 220(220
Suppl 2). 2019, S33–S41. - Rosenkranz, K. M., Arora, T. K., Termuhlen, P. M.,
Stain, S. C., Misra, S., Dent, D. and Nfonsam, V.
Diversity, Equity and Inclusion in Medicine: Why It
Matters and How do We Achieve It?. Journal of surgical
education. 2021, 78(4), 1058–1065. - Strakowski, S. M., Keck, P. E., Jr, Arnold, L. M.,
Collins, J., Wilson, R. M., Fleck, D. E., Corey, K. B.,
Amicone, J. and Adebimpe, V. R. Ethnicity and
diagnosis in patients with affective disorders. The Journal
of clinical psychiatry. 2003, 64(7), 747–754 - Gara, M. A., Vega, W. A., Arndt, S., Escamilla, M.,
Fleck, D. E., Lawson, W. B., Lesser, I., Neighbors, H.
W., Wilson, D. R., Arnold, L. M. and Strakowski, S. M.
Influence of patient race and ethnicity on clinical
assessment in patients with affective disorders. Archives
of general psychiatry. 2012, 69(6), 593–600 - Massie, J. P., Cho, D. Y., Kneib, C. J., Burns, J. R
Crowe, C. S., Lane, M., Shakir, A., Sobol, D. L., Sabin,
J., Sousa, J. D., Rodriguez, E. D., Satterwhite, T. and
Morrison, S. D. Patient Representation in Medical
Literature: Are We Appropriately Depicting Diversity?
Plastic and reconstructive surgery. Global open. 2019,
7(12), e2563. - Ooi, R., Lim, S., Ooi, S. and Bennett, A.
Representing Black, Asian and Minority Ethnic Skin in
Dermatology Education Amidst the COVID-19
Pandemic: An Evaluation of an E-learning Resource.
Cureus. 2021, 13(12), e20738. - Brennan M. Breast cancer in ethnic minority groups
in developed nations: Case studies of the United
Kingdom and Australia. Maturitas. 2017, 99, 16-19 - Ameh, C. A. and Van Den Broek, N. Increased risk
of maternal death among ethnic minority women in the
UK. The Obstetrician & Gynaecologist. 2008 10(3), 177
182. - Delon, C., Brown, K. F., Payne, N. W. S.,
Kotrotsios, Y., Vernon. S. and Shelton, J. Differences in
cancer incidence by broad ethnic group in England. Br J
Cancer. 2022, 2013–2017. - Knight, M., Bunch, K., Tuffnell, D., Patel, R.,
Shakespeare, J., Kotnis, R., Kenyon, S., Kurinczuk, J. J.
On behalf of MBRRACE-UK. Saving Lives, Improving
Mothers’ Care – Lessons learned to inform maternity care
from the UK and Ireland Confidential Enquiries into
Maternal Deaths and Morbidity 2017-19. Oxford-
National Perinatal Epidemiology Unit, University of
Oxford; 2021. - Davis, G. and Allison, R. White coats, Black
specialists? Racial divides in the medical profession,
Sociological Spectrum. 2013, 33(6), 510-533 - Roeder, A. America is failing its Black mothers,
Harvard Public Health Magazine, Retrieved June 1st
2022 from: [Internet]; 2019 [cited 2022, Nov 23].
Available from: https://www. hsph. harvard.
edu/magazine/magazine_article/america-is-failing-its-
black-mothers/ - Cho, D. Y., Kneib, C. J., Shakir, A., Burns, J. R.,
Lane, M., Massie, J. P., Crowe, C. S., Sobol, D. L.,
Morrison, S. D., Sousa, J. D. and Sabin, J.
Underrepresentation of Racial Minorities in Breast
Surgery Literature: A Call for Increased Diversity and
Inclusion. Annals of surgery. 2021, 273(2), 202-207 - Wen, D., Khan, S. M., Ji Xu, A., Ibrahim, H., Smith
L., Caballero, J., Zepeda, L., de Blas Perez, C.,
Denniston, A. K., Liu, X. and Matin, R. N.
Characteristics of publicly available skin cancer image
datasets: a systematic review. The Lancet. Digital health.
2022, 4(1), e64–e74. - Hereford, B., Kim, Y., Zaenglein, A. L. and Hollins,
L. C. Photographic representation of skin tones in three
dermatology journals. Pediatric dermatology. 2021, 38
Suppl 2, 146–148. - Garrick, J. F., Perez, B., Anaebere, T. C., Craine, P.,
Lyons, C. and Lee, T. The Diversity Snowball Effect:
The Quest to Increase Diversity in Emergency Medicine:
A Case Study of Highland’s Emergency Medicine Residency Program. Annals of emergency medicine.
2019. 73(6), 639–647. - Institute of Medical Illustrators. National Guidelines
[Internet]; 2022 [cited 2022, Mar 30]. Available
from:https://www. imi. org. uk/resources/professional-resources/national-guidelines/ - Association of Medical Illustrators (2022). History
of medical illustration [Internet]; 2022, May [cited 2022
May 10]. Available from: https://ami. org/professional
resources/advocacy/legal-news/27-main/medical
illustration/49-history-of-medical-illustration - Louie, P. and Wilkes, R. Representations of race and
skin tone in medical textbook imagery. Social science &
medicine. 2018, 202, 38–42. - Adelekun, A., Onyekaba, G. and Lipoff, J. B. Skin
color in dermatology textbooks: An updated evaluation
and analysis. Journal of the American Academy of
Dermatology. 2021, 84(1), 194–196. - Gwan, A., Tanner-Sanders, L. N., Nair, N., Chapple,
A. G. and Jernigan, A. Equity in visual representation of
vulvar conditions in major gynecology textbooks. Journal
of the National Medical Association. 2022, S0027
9684(22)00037-2. - El Saadawi, N. Taw’am al-salta wa’l jins. Windsor,
UK: Hindawi Foundation C. I. C.; 2017. - Ibn Adam, M. A Detailed Exposition of the Fiqh of
Covering One’s Nakedness (awra) in Hanafi Fiqh
[Internet]; 2010, Sep 19 (cited 2022, May 10). Available
from: https://seekersguidance. org/answers/hanafi-fiqh/a-
detailed-exposition-of-the-fiqh-of-covering-ones-
nakedness-awra/ - Saidun, S. Photographing human subjects in
biomedical disciplines: an Islamic perspective. J Med
Ethics. 2013, 39(2), 84-8. - Maravia, U. and Al-Ghazal, S. K. Bimaristans:
Services and educational role in Islamic medical history
and their influence on modern medicine and hospitals.
JBIMA. 2021, 8(3), 1-15. - Haneef, S. S. S. Modern Means of Proof: Legal
Basis for Its Accommodation in Islamic Law. Arab Law
Quarterly. 2006, 20(4), 334-364. - Al-Mutee’i, M. B. Al-jawab al-shafi fi ibahat at-
tasweer al-fotografi. Cairo, Egypt: al-Matba’a al-
Khayriyya; 1881. - Ibn Abideen, M. A. Radd al-muhtar ala’d durr al-
mukhtar (vol. 3). Beirut, Lebanon: Dar al-Fikr; 1992
